Reduction of a Hyper-kyphosis in a 16-year-old female patient using a 3D designed kyphosis brace
Case Background
The patient presented to the ScoliCare clinic at 14 years of age with postural deformity and pain in the middle back.
Examination Findings
The patient was a pre-menarchal teenager who reported pain across the shoulder blades that extended from the upper thoracic spine down to the lower lumbar spine. The patient rated their pain as 6/10 on a visual analogue scale and stated that the pain and stiffness in their back was impacting on their daily activities. The patient was otherwise healthy. The physical examination revealed a significant increase in the patient’s thoracic kyphosis and lumbar lordosis (Figure 1), with marked angulation of the thoracolumbar spine during forward bending. There were no other significant clinical findings. A provisional diagnosis of Scheuermann’s kyphosis was made and confirmatory imaging was requested. Plain films taken soon after the examination highlighted an abnormal curvature in the sagittal plane – specifically a 67° hyper-kyphosis in the thoracic spine with an apex at T10. There was notable wedging of the T10 & T11 vertebrae in the lower thoracic spine.
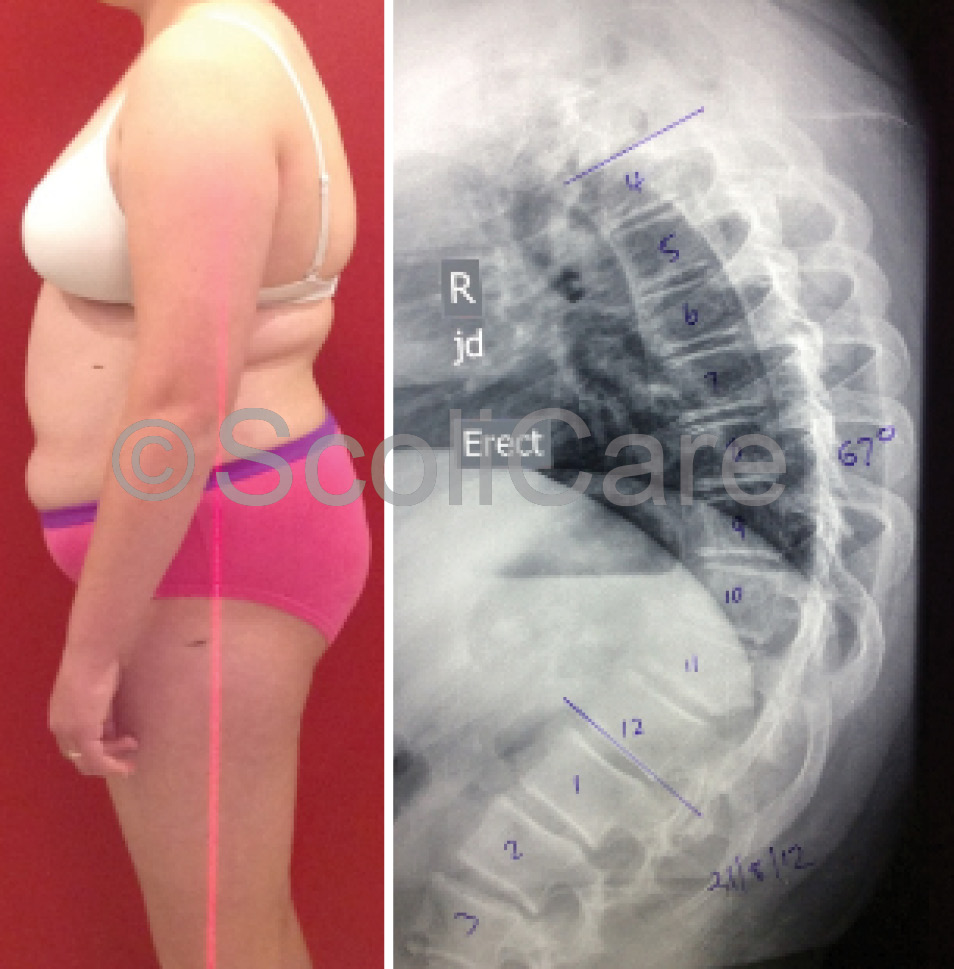
Lateral x-ray indicating a hyper-kyphosis (Right)
Intervention
The patient was prescribed a customised 3D designed rigid kyphosis brace and specific exercise rehabilitation to address the spinal deformity. The patient was advised to wear the brace for 20 hours per day for a period of 18 months. With respect to the exercise rehabilitation, specific exercises were given to strengthen the spinal extensors. The exercises were administered during one-on-one sessions with an exercise physiologist initially, then the patient was instructed to perform these exercises daily at home to complement the action of the brace. Exercises were modified and/or progressed as the patient’s strength and endurance improved.
Outcomes
In-brace x-rays were taken one month after the brace fitting which indicated that the curve could be reduced from 67° down to 42° whilst wearing the brace (Figure 2).
After three months of brace wear an x-ray was taken with an independent radiology clinic. The images were taken with the patient standing in their normal relaxed posture after being out of the brace for 12 hours. These x-rays demonstrated a reduction in the curve from 67° down to 54°.
The patient wore the brace and continued the exercises for a further 12 months. Brace weaning was initiated after 15 months of brace wear. Plain films taken at the end of the brace weaning period revealed that the curve had remained stable at 54° (Figure 3). The patient was instructed to continue with the exercise rehabilitation after the cessation of brace wear, with the expectation that if the patient keeps up with their exercise program that their curve will remain under 60°.


Lateral x-ray indicating 54° thoracic kyphosis after the brace fitting
Discussion
The normal angle of kyphosis in young patients ranges from 20-45°. One condition that may alter the normal thoracic curvature is Scheuermann’s disease. Classified as one of the osteochondroses, Scheuermann’s disease usually appears just prior to puberty with roughly equal prevalence between males and females. The condition is characterised by an increase in the normal thoracic kyphosis and is associated with structural changes in the vertebral bodies – namely wedging, endplate irregularities and diminished anterior vertebral body growth.
Long-term follow-up studies highlight that patients with Scheuermann’s disease tend to have more severe back pain, work lighter jobs and have more concerns regarding their appearance when compared with healthy patients. If left untreated, patients with kyphosis tend to experience a progression of their deformity and associated back pain. The scientific literature points to bracing being an effective treatment for patients with hyper-kyphosis. Bracing appears to not only prevent progression in this group but may also serve to restore the normal kyphosis in some patients. The best results from bracing are observed when treatment is initiated in skeletally immature patients who have curvatures of between 55-80°.
Conclusion
This case demonstrates the successful management of an adolescent patient with hyper-kyphosis using a customised 3D designed rigid kyphosis brace and specific exercise rehabilitation.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.
© ScoliCare & The ScoliCare Clinic Sydney